The 2022 European Society of Cardiology/European Respiratory Society (ESC/ERS) guidelines redefined pulmonary hypertension (PH) as a mean pulmonary arterial pressure (mPAP)>20 mmHg.1) This update is supported by the evidence that prognosis was poor with mPAP ≥19 mmHg in adults.2–4) The guidelines recommend applying this criterion to pediatric patients, but treatment and prognosis in children with mild PH remain unclear. This study aimed to investigate the characteristics and clinical course of pediatric patients with mild PH.
Study Design
This retrospective observational study was conducted at a single center. Our hospital serves the northern and the eastern regions of Hokkaido and is the only facility that undertakes pediatric cardiac catheterization in these areas.
Inclusion criteria are as follows; 1) patients aged ≤18 years at their initial cardiac catheterization, and 2) patients whose mPAP have been measured as between 20 mmHg and 25 mmHg on cardiac catheterization. The exclusion criteria are; 1) patients with single-ventricular physiology, 2) patients with pulmonary stenosis and lung perfusion distribution of <0.5 on lung perfusion scintigraphy, and 3) patients with pulmonary venous stenosis.
Clinical Data
We retrospectively reviewed the clinical data extracted from the medical records of all pediatric patients who visited our hospital and underwent cardiac catheterization between January 2005 and December 2022.
Procedures and Definitions
Cardiac catheterization was performed under transvenous anesthesia with spontaneous breathing. Occasionally, we used the jaw-thrust maneuver or a nasotracheal airway for respiratory support under sedation. We avoided use of oxygen. mPAP was calculated as an average of the right and the left pulmonary arterial pressures. Pulmonary arterial wedge pressure (PAWP) was calculated as an average of the right and the left PAWPs. For mPAP and PAWP, the absolute difference between the left and the right pressures measured was calculated to evaluate the left-right difference. Diastolic pressure gradient (DPG) was calculated using the formula; diastolic pulmonary arterial pressure – PAWP.
In patients in whom a catheter tip could reach the left atrial cavity via the right atrium and an inter-atrial communication, we used the pulmonary venous pressure as a substitute for PAWP. Systemic and pulmonary blood flow were both measured using the Fick method.
Measurements of mPAP between 20 mmHg and 25 mmHg and those ≥25 mmHg were defined as mild PH and traditional PH, respectively, as determined on cardiac catheterization. Hemodynamic definitions of PH were classified using mPAP, PAWP, and pulmonary vascular resistance index (PVRI), as per recent guidelines.1) That is, PH with PAWP <15 mmHg and PVRI ≥3 WU·m2 was defined as pre-capillary PH, PH with PAWP ≥15 mmHg and PVRI <3 WU·m2 was defined as isolated post-capillary PH, PH with PAWP ≥15 mmHg and PVRI ≥3 WU·m2 was defined as combined pre- and post-capillary PH, and PH with PAWP <15 mmHg and PVRI <3 WU·m2 was defined as unclassified PH.
Patients diagnosed as having PH and subsequently re-evaluated on cardiac catheterization were divided into two groups: Cohort I (improved; as mPAP decreased over time) and Cohort W (worsened; as mPAP increased over time). In those patients who underwent cardiac catheterization more than once, we recorded the data from the latest examination that had been performed.
Statistical Analyses
Categorical variables were expressed as numbers (percentages) and analysed using the chi-square test. Continuous variables were expressed as medians (interquartile ranges) and analysed using the Mann–Whitney U-test. Time series data on catheterization were analysed using Wilcoxon’s signed rank test. Statistical significance was set at p<0.05.
Study Population
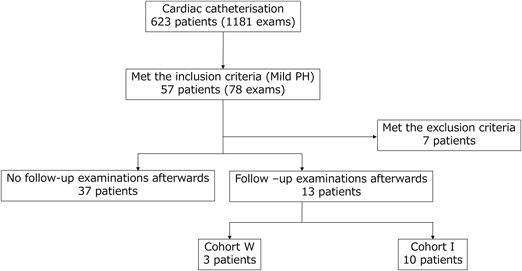
During the study period, 1181 cardiac catheterizations were performed in 623 patients. The number of exams that met the definitions of traditional and mild PH were 159 (13.5%), and 78 (6.6%), respectively. There was no report of death among the patients with traditional or mild PH. Among the 78 exams (in 57 patients), 7 patients met the exclusion criteria, and 37 patients had not undergone subsequent cardiac catheterization. Thus, the remaining 13 patients were enrolled into the two groups: Cohort W (n=3), and Cohort I (n=10) (Fig. 1).
The median period between the two catheterization dates for each patient was 65 (34–86) months. Except for two patients with mild PH, the rest had concomitant congenital heart diseases (supplementary data). Among the study population, no reported cases met the criteria for mild PH of idiopathic or heritable pulmonary arterial hypertension, connective tissue disease, portal hypertension, persistent PH of the newborn, bronchopulmonary dysplasia, or chronic thromboembolic PH. The absolute difference between the left and the right mPAP and PAWP ranged from 0 to 3 and 0 to 2, respectively. The two patients who exhibited a 3-mmHg left-right difference in mPAP underwent pulmonary perfusion scintigraphy, which confirmed that they did not meet the aforementioned exclusion criteria. Furthermore, no patient exhibited segmental PH in which one lung met the diagnostic criteria for PH but the other did not.
Comparative Analyses between the Two Cohorts
The demographic and clinical characteristics of the two groups are presented in Table 1. Age at diagnosis of mild PH in Cohort I was significantly lower than that in Cohort W. The number of patients with heart valve disease of the left side was significantly larger in Cohort W. On the other hand, 4 patients in Cohort I had congenital heart diseases with increased pulmonary blood flow, and subsequently underwent intracardiac repair. Pulmonary vasodilators were used in 2 patients with hemodynamic pre-capillary PH because they were clinically determined to have traditional PH during the period after intracardiac repair and before a diagnosis of mild PH (supplementary data).
Table 1 Patients’ characteristics who met the criteria of mild PH| Item | Cohort W | Cohort I | p value |
|---|
| Total number of patients (N) | 3 | 10 | |
| Age (years) | 7.2 (6.3–15.3) | 1.0 (0.7–5.4) | 0.036 |
| Gender (M/F) | 1/2 | 6/4 | 0.42 |
| Chromosomal disorders |
| Trisomy 21 | 1 (33%) | 3 (30%) | 0.91 |
| Pulmonary/systemic blood flow ratio |
| <1.0 | 0 | 2 (20%) | 0.4 |
| =1.0 | 3 (100%) | 4 (40%) | 0.067 |
| >1.0 | 0 | 4 (40%) | 0.19 |
| Valve disease of the left heart | 2 (67%) | 1 (10%) | 0.041 |
| Mitral valve regurgitation | 2 | 0 | |
| Aortic stenosis | 0 | 0 | |
| Aortic valve regurgitation | 0 | 1 | |
| Cardiomyopathy |
| Restrictive cardiomyopathy | 1 (33%) | 0 | 0.057 |
| Respiratory disease | 1 (33%) | 1 (10%) | 0.33 |
| Congenital diaphragmatic hernia | 0 | 1 | |
| Pulmonary lymphangiectasis | 1 | 0 | |
| Arrhythmias | 0 | 0 | |
| Hemodynamic definitions |
| Pre-capillary PH | 1 (33%) | 6 (60%) | 0.42 |
| Isolated post-capillary PH | 1 (33%) | 2 (20%) | 0.63 |
| Combined pre- and post-capillary PH | 0 | 0 | |
| Unclassified PH | 1 (33%) | 2 (20%) | 0.63 |
| Treatment |
| Pulmonary vasodilator | 1 (33%) | 1 (10%) | 0.33 |
| Surgery | 1 (33%) | 6 (60%) | 0.42 |
| Values are presented as counts (%). Age is presented as median (interquartile range). PH, pulmonary hypertension |
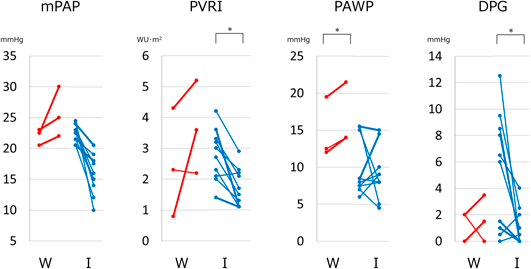
Data regarding cardiac catheterizations are depicted in Fig. 2. The PVRI and DPG decreased significantly in Cohort I (p=0.0012 and p=0.013, respectively). The PAWP increased significantly in Cohort W, whereas no change in Cohort I (p=0.0082 versus p=0.615, respectively).
Characteristics of the Patients in Cohort W
Details of the 3 patients in Cohort W are depicted in Table 2. Notably, the PAWP was ≥12 mmHg at the time of diagnosis with mild PH in these cases. They exhibited pathogenic conditions that could have increased PAWP. Patient No. 1, and No. 3 had moderate mitral valve regurgitations (MR), and Patient No. 2 had restrictive cardiomyopathy (RCM). These impediments are known causes of post-capillary PH, suggesting that elevated mPAP was strongly associated with their underlying left heart disease.
Table 2 Characteristics of three patients in Cohort W| Patient No. | Initial diagnosis | Age (years) | Gender | Surgery | mPAP (mmHg) | PVRI (WU·m2) | PAWP (mmHg) | DPG (mmHg) |
|---|
| Complications |
|---|
| 1 | T21, TOF, PLA | 15.3 | M | TOF repair | 23 | 4.3 | 12 | 2 |
| MR (moderate) | 21.1 | PVR | 25 | 5.2 | 14 | 3.5 |
| 2 | RCM | 7.2 | F | | 22.5 | 0.8 | 19.5 | 0 |
| 10.0 | | 30 | 3.6 | 21.5 | 1.5 |
| 3 | PDA | 6.3 | F | PDA ligation | 21 | 2.3 | 12.5 | 2 |
| MR (moderate) | 9.3 | | 22 | 2.2 | 14 | 0 |
| The upper row of each table shows the earlier data, and the lower row the later data. DPG, diastolic pressure gradient; mPAP, mean pulmonary artery pressure; MR, mitral valve regurgitation; PAWP, pulmonary artery wedge pressure; PDA, patent ductus arteriosus; PLA, pulmonary lymphangiectasis; PVR, pulmonary valve replacement; PVRI, pulmonary vascular resistance index; RCM, restrictive cardiomyopathy; T21, Trisomy 21; TOF, tetralogy of Fallot; WU, Wood unit |
|---|
Summary and Significance of the Main Findings
This is the first study to elucidate the characteristics and clinical courses of pediatric mild PH, as per the current 2022 ESC/ERS guidelines.1) We found that pediatric mild PH frequently improved over time. An increase in mPAP over time was seen in 23% (n=3) of patients. These 3 patients had three characteristics; 1) a relatively older age at the time of diagnosis of mild PH, 2) PAWP increasing with age, and 3) PAWP ≥12 mmHg at the time of diagnosis of mild PH. Because the upper limit of normal PAWP is considered to be 12 mmHg, their PAWP is considered high.1) All of them had left heart diseases, namely moderate MR or RCM, which are established etiologies of post-capillary PH. Our study highlights that elevated PAWP (≥12 mmHg) in the setting of left or systemic heart disease can be an indicator of subsequent worsening PH even in the pediatric population, underlining the need for careful follow-up in this subgroup.
Comparison with the Findings in Previous Studies
Blood vessels change structurally and functionally with advancing age in adults, resulting in increased stiffness, vascular wall remodelling, and loss of angiogenic ability.5) Conversely, pediatric pulmonary vessels are expected to grow with age6) and have “high reversal potential from PH” etiology.7) For instance, successful repair of a left-to-right shunt lesion, when established before structural remodelling became irreversible, would alleviate mechanical stress on the pulmonary vessels.
Our study showed that mild PH improved in most pediatric patients. Still, mPAP increased over time in some pediatric patients having PH associated with unresolved left or systemic heart disease. In such circumstances, elevation of PAWP coexisted, although the criterion for post-capillary PH (PAWP ≥15 mmHg) was not necessarily fulfilled. Pulmonary vasodilators are considered ineffective or even harmful in adult patients with PH who have left heart disease. In addition, effective drug therapy targeting the pulmonary vasculature has not been established.8) The management of pediatric PH with heart disease of the systemic ventricle is also considered extremely challenging.9) Therefore, careful follow-up is essential in patients with pathologies resulting in high PAWP.
Study Limitations
This study had a few limitations. First, this was a single-center retrospective study, and inclusion of individuals only from a certain local region of Japan may have introduced a selection bias. Second, 37 patients with mild PH did not undergo subsequent cardiac catheterization because they did not meet the traditional criteria and, therefore, were not scheduled for a re-evaluation. Third, the maximum follow-up period in this study was 17 years; therefore, it was inappropriate for us to discuss the prognosis of pediatric mild PH throughout adulthood. Finally, these patients were not investigated by means of pulmonary histopathological analysis or genetic tests.
This study revealed that mild PH in the majority of pediatric patients improved over time. Some patients showed an increase in mPAP; this phenomenon coincided with elevated PAWP. Patients with PAWP elevated (≥12 mmHg) should receive careful follow-up to prevent worsening of PH.
Conflicts of Interest
The authors have no competing interests.
Data Availability
The data sets analysed during the current study are included in this published article and its supplementary information files.
Author Contribution
Conceptualization: Sorachi Shimada. Data curation: Sorachi Shimada. Methodology: Sorachi Shimada. Investigation: Sorachi Shimada. Project administration: Sorachi Shimada and Kouichi Nakau. Supervision: Kouichi Nakau and Satoru Takahashi. Writing-original draft: Sorachi Shimada. Writing-review & editing: Kouichi Nakau, Yuki Shibagaki, Keita Ito, Yuki Sasaki, Rina Imanishi, Hideharu Oka, and Satoru Takahashi. Validation: Kouichi Nakau, Yuki Shibagaki, Keita Ito, Yuki Sasaki, Rina Imanishi, Hideharu Oka, and Satoru Takahashi. Formal analysis: Kouichi Nakau, Yuki Shibagaki, Keita Ito, Yuki Sasaki, Rina Imanishi, and Hideharu Oka.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles set out in the Code of Ethics of the World Medical Association, 1975 Declaration of Helsinki, and it was approved by the ethics committee of our hospital (approval no. 24055).
Patient Declaration of Consent Statement
The requirement for informed consent was waived owing to the retrospective nature of the study.
Note
Supplemental date is provided online for this article.
引用文献References
1) Humbert M, Kovacs G, Hoeper MM, et al: ESC/ERS Scientific Document Group: 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2022; 43: 3618–3731
2) Maron BA, Hess E, Maddox TM, et al: Association of borderline pulmonary hypertension with mortality and hospitalization in a large patient cohort: Insights from the Veterans Affairs clinical assessment, reporting, and tracking program. Circulation 2016; 133: 1240–1248
3) Kolte D, Lakshmanan S, Jankowich MD, et al: Mild pulmonary hypertension is associated with increased mortality: A systematic review and meta-analysis. J Am Heart Assoc 2018; 7: e009729
4) Douschan P, Kovacs G, Avian A, et al: Mild elevation of pulmonary arterial pressure as a predictor of mortality. Am J Respir Crit Care Med 2018; 197: 509–516
5) Dieffenbach PB, Aravamudhan A, Fredenburgh LE, et al: The mechanobiology of vascular remodeling in the aging lung. Physiology (Bethesda) 2022; 37: 28–38
6) Dias R, Saini AS, O’Dell W: Assessing lung vasculature development and application to early preterm gestation patients. J Undergrad Res (Gainesv) 2022; 24
7) Kulik TJ, Austin ED: Pulmonary hypertension’s variegated landscape: A snapshot. Pulm Circ 2017; 7: 67–81
8) Maron BA, Bortman G, De Marco T, et al: Pulmonary hypertension associated with left heart disease. Eur Respir J 2024; 64: 2401344
9) Patten WF, Krishnan US: Pediatric pulmonary hypertension in left-sided heart disease. Adv Pulm Hypertens 2023; 22: 134–139
 *1,Kouichi Nakau,Yuki Shibagaki,Keita Ito,Yuki Sasaki,Rina Imanishi,Hideharu Oka,Satoru TakahashiSorachi Shimada
*1,Kouichi Nakau,Yuki Shibagaki,Keita Ito,Yuki Sasaki,Rina Imanishi,Hideharu Oka,Satoru TakahashiSorachi Shimada