Patient: A 4-month-old male.
Perinatal history: The patient was born at 39 weeks and 1 day via a spontaneous delivery by a local obstetrician, birth weight being 3,002 g. The Apgar scores were 8 at 1 minute and 10 at 5 minutes.
Past medical history: On the fourth day of life, the patient was diagnosed with a small ventricular septal defect (VSD) within the membranous part of the ventricular septum. At 1 month of age, the defect remained patent, and a re-examination was scheduled at 4 months of age.
No relevant family history.
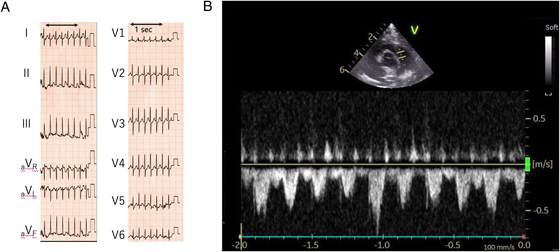
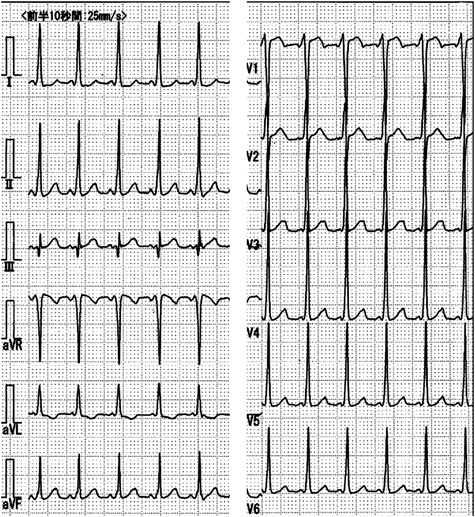
Current medical history: At 4 months of age, the patient re-visited his initial physician for a routine VSD checkup. During echocardiography to evaluate the VSD, his HR accelerated markedly with crying. The HR elevation appeared not to be attributed solely to sinus tachycardia associated with crying. As a precise measurement was challenging, the waveform of blood flow velocity across the main pulmonary artery was assessed using the pulse-wave Doppler method. The circumstance was confirmed with 12-lead ECG (Fig. 1A, B). His HR exceeded 300 beats/minute, prompting transfer to our hospital for further evaluation of the tachyarrhythmia.
On arrival, the patient was 64 cm tall (−0.1 SD), weighed 6.6 kg (−0.6 SD), and had HR 250 beats/minute, blood pressure 115/74 mmHg, respiratory rate 40 breaths/min, body temperature 36.8°C, and SpO2 100% on room air. His heart sounds were clear, with no murmurs detected. The patient was conscious, with a normal breathing pattern and sounds, warm extremities, and no signs of distress.
Examination findings on arrival: A simple chest X-ray showed a cardiothoracic ratio (CTR) of 50%, with no evidence of pneumonia or congestion (Fig. 2). Blood tests revealed no particular abnormalities in electrolytes or thyroid function (Table 1).
Table 1 Blood test results on arrival at our hospital| blood count | biochemistry | venous blood gas |
|---|
| WBC | 17.8×10^3 | /μL | AST | 31 | U/L | pH | 7.458 | |
| RBC | 5.15×10^6 | /μL | ALT | 29 | U/L | pCO2 | 28 | mmHg |
| Hgb | 10.9 | g/dL | LDH | 210 | IU/L | pO2 | 49.2 | mmHg |
| Hct | 41 | % | CK | 102 | U/L | BE | −3 | mmol/L |
| Plt | 592×10^3 | /μL | CK-MB | 1.09 | U/L | HCO3- | 19.4 | mmol/L |
| Neutro (%) | 61.2 | % | UN | 8 | mg/dL | Lac | 3.64 | mmol/L |
| Lymph (%) | 30.4 | % | Cre | 0.2 | mg/dL | | | |
| Eo (%) | 1.5 | % | UA | 3.8 | mg/dL | | | |
| | | Ca | 11.1 | mg/dL | | | |
| | | P | 6.3 | mg/dL | | | |
| | | Mg | 2.1 | mg/dL | | | |
| | | Na | 140 | mEq/L | | | |
| | | K | 5 | mEq/L | | | |
| | | Cl | 105 | mEq/L | | | |
| | | CRP | 0.56 | mg/dL | | | |
| | | TSH | 2.49 | μIU/mL | | | |
| | | fT3 | 5.04 | pg/mL | | | |
| | | fT4 | 1.33 | ng/mL | | | |
| | | NT-proBNP | 457.8 | pg/mL | | | |
| The N-terminal pro B-type natriuretic peptide level was mildly elevated, whereas no elevations in the myocardial deviation enzymes were observed. No electrolyte abnormalities, nor thyroid function abnormalities, either. |
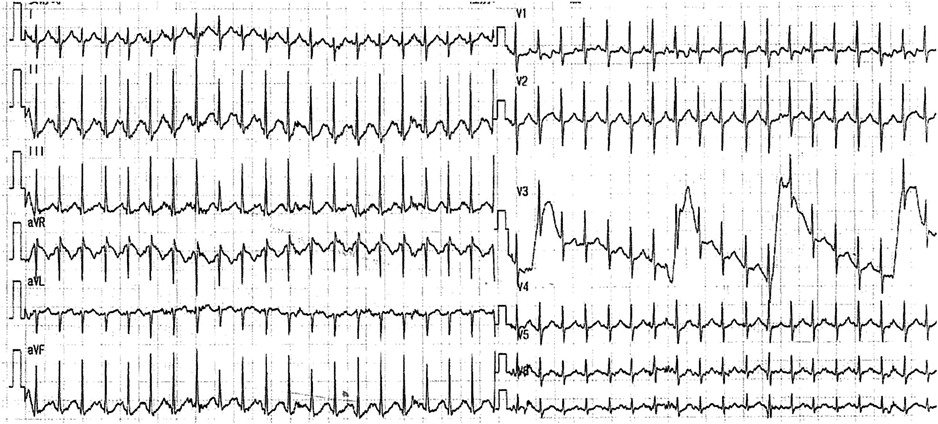
Clinical course after hospitalization: As mentioned above, 12-lead ECG performed by the previous physician revealed a marked tachycardia with an HR of 326 beats/minute. Initially, the patient was suspected to have a narrow QRS tachycardia with an unclear P wave and a constant RR interval, leading to a provisional diagnosis of atrioventricular reciprocating tachycardia (AVRT). 12-lead ECG performed upon arrival at our hospital revealed HR of 250 beats/minute, lower than the previously recorded figure. Still, the tachycardia persisted. Similar to the previous findings, the updated 12-lead ECG displayed a narrow QRS tachycardia with a constant RR interval. P wave was clearly observed preceding QRS wave, and there was no delta (Δ) wave (Fig. 3).
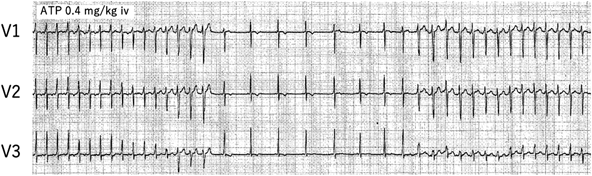
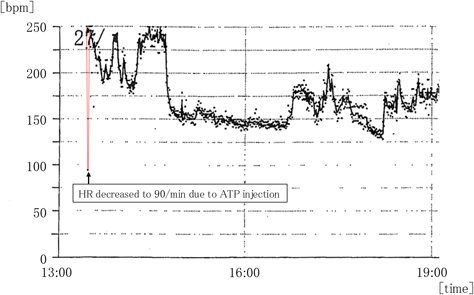
For an arrhythmia diagnosis, ATP was administered intravenously at 0.2 mg/kg. No atrioventricular block occurred following the ATP administration, while a Δ wave appeared. A bolus injection of 0.4 mg/kg of ATP terminated the tachycardia, and sinus rhythm resumed at 90 beats/minute without atrioventricular block. Shortly thereafter, however, HR went up to 250 beats/minute with Δ wave (Fig. 4). After the recurrence of tachycardia, HR fluctuated between 180 and 250 beats/minute and eventually recovered to normal sinus rhythm with an HR of around 160 beats/minute two hours after arrival at our hospital. The HR trend on Holter monitoring showed sudden termination of this tachycardia (Fig. 5). AVRT with retrograde accessory conduction pathways was suspected due to the significantly elevated HR at the onset of the episode, and the subsequent appearance of Δ wave after ATP administration. Flecainide was initiated at 4 mg/kg/day orally, although his tachycardia had already ceased at the time of the first oral administration. The Δ wave on resting ECG led to a diagnosis of Type B WPW syndrome (Fig. 6). Furthermore, an ATP administration suppressed the ectopic rhythm, restored sinus rhythm, and clarified the diagnosis as AT complicated by WPW syndrome. Flecainide was considered effective for the AT, and the patient stayed on the drug treatment. During the hospitalization, there was no evidence of tachycardia-induced cardiomyopathy. The patient was followed every 2 to 6 months for 1 year without any recurrence of arrhythmias.
This case highlighted two key points: (1) The patient experienced a tachycardia attack when crying intensely on periodic echocardiography, and the physician suspected that it was unlikely sinus tachycardia associated with crying. (2) Based on the changes in tachycardia HRs and ECG findings, a diagnosis of AT was made even with the presence of Δ wave.
Recognition of a Tachycardia Attack
The patient began crying soon after starting echocardiography examination, and HR appeared abnormally fast for crying. This led to a diagnosis of tachyarrhythmia. In pediatric practice, crying and associated transient tachycardia are commonly observed during evaluations. With sinus tachycardia in fetuses and infants, HR can briefly rise to approximately 230 beats/minute.1) When HR significantly exceeds this threshold, even during crying, a tachyarrhythmia should be suspected and investigated. In this patient, no hypotension or symptoms associated with heart failure were observed during the tachycardia with HR over 300 beats/minute, and his condition did not deteriorate until the tachycardia was converted to sinus rhythm 4 hours and 30 minutes after recognition of the tachycardia. It is generally challenging to determine whether HR exceeds 200–230 beats/minute or not through auscultation and visual inspection during echocardiography. For instance, rates of 180 and 240 beats/minute correspond to 3 and 4 beats/second, respectively, making them difficult to differentiate during examination. In our patient, tachycardia did not present as a primary complaint. Instead, tachyarrhythmia was diagnosed when his HR during crying was suspected to deviate from sinus tachycardia typically associated with crying.
HR >200 beats/minute during a tachycardia attack poses a high risk for progression to congestive heart failure.1) Active diagnostic measures, such as 12-lead ECG, prolonged ECG monitoring, Holter ECG, and drug loading, are essential when distinguishing between tachyarrhythmias and sinus tachycardia. Additionally, pulmonary arterial blood flow velocity quantification using Doppler imaging can provide valuable diagnostic insight on echocardiography, as performed in this case.
Differentiation of Tachyarrhythmia
In this case, a preceding P wave was observed during the tachycardia at a heart rate of 250 beats/minute, and Δ wave became apparent after ATP administration. It is likely because conduction through an accessory pathway was unmasked due to suppression of normal atrioventricular conduction. Additionally, high-dose ATP suppressed fast P wave (HR >250 beats/minute) and slower P wave (HR around 90 beats/minute) emerged, suggesting that the ATP-sensitive AT was temporarily suppressed. This allowed a transient return to sinus rhythm with a WPW syndrome pattern.
On the other hand, alternative forms of tachycardia should also be considered. The narrow QRS tachycardia with HR of 326 beats/minute may represent AVRT via an accessory pathway, because of the varying HR and potential existence of P wave just after the QRS complex during tachycardia. Another possible mechanism is that tachycardia with HR of 250 beats/minute represents inappropriate sinus tachycardia, as the P wave morphology during tachycardia (Fig. 3) closely resembles that during sinus rhythm (Fig. 6); I, II (+), III (±), aVR (−), aVL (+), aVF (+), V4–V6 (+). We diagnosed this tachycardia as AT, because HR was excessively rapid to be classified as sinus tachycardia, and HR trend on Holter ECG showed warm-up and cool-down, suggesting the arrythmia was most likely due to AT.
In Fig. 4, the QRS complex became more pre-excited just before the termination of the tachycardia, which may explain the inhibition of normal atrioventricular conduction during ATP infusion, but in the process of termination of the tachycardia, the QRS became narrower before the tachycardia really terminated; it was possibly due to acceleration of junctional rhythm. Nonetheless, inappropriate sinus tachycardia cannot be ruled out definitively as a differential diagnosis for atrial tachycardia originating from a site adjacent to the sinus node.
Regardless of whether such tachycardia is of a sinus or an atrial pattern, the tachycardia itself may cause cardiac ischemia and lead to life-threatening arrhythmias in infants because of a very rapid HR.2) Focal AT is the most frequent underlying cause of tachycardia-induced cardiomyopathy in childhood.3) Furthermore, the incidence of tachycardia-induced cardiomyopathy is significantly higher in patients aged ≤4 months.4) Therefore, careful follow-up is critical. If the condition in our patient would be refractory to medical therapy, further evaluation on electrophysiological study and catheter ablation should be considered.
 1,2,Kodai Momoki2,Susumu Hosokawa3,Kenji Hoshino1,2,Satoshi Masutani4,5,6,Naokata Sumitomo5Emi Kittaka
1,2,Kodai Momoki2,Susumu Hosokawa3,Kenji Hoshino1,2,Satoshi Masutani4,5,6,Naokata Sumitomo5Emi Kittaka