Pectus excavatum is characterized by a depressed sternum, narrowed mediastinum, compressed heart, and impaired pulmonary function. Most patients remain asymptomatic and may undergo surgery for cosmetic reasons, while Fontan candidates may require correction of pectus excavatum to avoid compression of a conduit route or the pulmonary vein and thus to establish a good Fontan circulation. Here, we present a case of successful simultaneous surgery of modified Nuss procedure and total cavopulmonary connection (TCPC) surgery.
A 2-year-old girl with right isomerism and functional single ventricle, who had undergone the Glenn procedure at 1 year old, was scheduled for completion of TCPC.
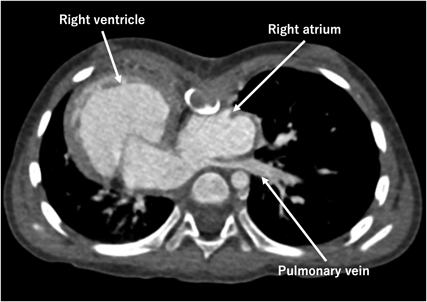
Preoperative computed tomography scan revealed compression of the right atrium and the left pulmonary vein by a depressed sternum, with the Haller Index of 6.25 (Fig. 1).
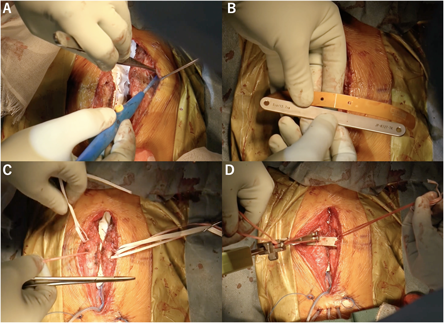
Due to concern regarding postoperative conduit obstruction and further impact on the pulmonary vein or the IVC (inferior vena cava), simultaneous modified Nuss procedure and Fontan completion were planned. The operation was performed via a redo median sternotomy under normothermic cardiopulmonary bypass. An 18 mm ePTFE conduit was used for the TCPC. After weaning from cardiopulmonary bypass, dissection was carried out anterior to the most indented site of the sternum and to the costal cartilage in order to create a pocket for a pectus bar. A soft template bar was pre-shaped to guide the bending of the 5-inch pectus bar. NESPLON cables (Alfresa Pharma, JAPAN) were passed around the costal cartilage on both sides of the sternum. After sternal closure with wires, the 5-inch pectus bar was inserted into the prepared pocket. The NESPLON cables were then tightened and pulled up. This maneuver elevated and corrected the sternum and the costal cartilages (Fig. 2; Video 1).
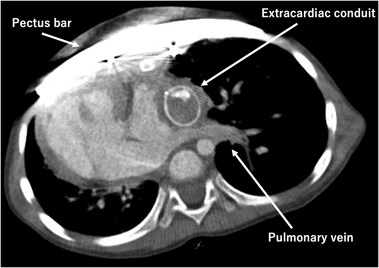
The postoperative course was uneventful, and the patient was discharged home on the 15th postoperative day. Postoperative computed tomography scan revealed repaired pectus excavatum without compression of the conduit, the IVC, nor the pulmonary veins. Haller index improved to 2.80 (Fig. 3).
The Nuss procedure is commonly performed between the ages of 10 and 18 years. Since the sternum of young children is soft, performing the Nuss procedure at an early age may lead to recurrence of pectus excavatum after removal of the pectus bar. Therefore, a two-stage repair, rather than a simultaneous approach as demonstrated in this case, would allow patients to undergo the Nuss procedure at the optimal age. When a two-stage approach is applied, on the other hand, adhesion within the mediastinum might increase a surgical risk and adverse events would occur more likely such as injury to the heart, the lungs, and collateral blood vessels during pectus bar insertion. Thus, the optimal surgical strategy remains controversial whether cardiac disease and pectus excavatum are to be repaired in a single-staged or a two-staged way. Of note, Park et al. and Yoshida et al. recently reported favorable outcomes of the Nuss procedure in patients before puberty.1, 2) They proposed that repairing pectus excavatum in younger patients may have several advantages. Yoshida and colleges revealed that younger patients tended to have a symmetric deformity and that asymmetric deformity progressed in older patients. Consequently, younger patients have a lower risk of bar displacement and exhibit more flexibility and symmetry of the chest wall contributing to a less complex surgical procedure.1)
In addition, the timing of removing the bar is crucial. Several studies demonstrated low recurrence rates of chest deformity in patients undergoing the Nuss procedure before puberty when the pectus bar was removed 2 to 3 years postoperatively, which was planned in our case. Nuss et al. revealed low recurrence rate when the bar was removed beyond more than 2 years after implantation.3) Similarly, Park et al. removed the bar after 2 years of placement and reported a recurrence rate of only 0.4%.1)
In our case, simultaneous repair was considered necessary to secure the Fontan pathway by correcting the pectus excavatum; compression to the Fontan route and the pulmonary veins were avoided. As anticipated preoperatively, postoperative CT revealed that the Fontan conduit occupied a considerable space within the thoracic cavity. The pulmonary veins appear better structured than preoperative state.
Nonetheless, perioperative management may be an issue. Nakahara et al. reported that cardiopulmonary resuscitation is challenging after the original Nuss procedure.4) They found that presence of a rigid pectus bar resulted in ineffective cardiac massage. They emphasized that management of arrhythmia is critical during perioperative period. Their experience raised a concern regarding safety of simultaneous repairs since cardiac surgery generally increases a risk of fatal arrhythmia. To address this issue, we placed the pectus bar anteriorly to the sternum (modified Nuss procedure) during sternal closure. This approach would facilitate easier removal of the pectus bar in the event of perioperative cardiopulmonary resuscitation; by swiftly reopening the surgical wound and simply extracting the pectus bar.
In addition, simultaneous repair may offer several advantages to Fontan patients during the perioperative period. Kawamura et al. reported that this approach can significantly reduce the risk of cardiac compartment syndrome related to sternum deformity.5) Maagaard et al. and Lawson et al. reported that repairing pectus excavatum improves both cardiac and pulmonary functions.6, 7) Consequently, simultaneous repair can provide beneficial circumstances by improving cardiopulmonary function.
We present a case of simultaneous surgery of the modified Nuss procedure and Fontan completion. To dismiss concerns regarding obstruction across the Fontan route due to pectus excavatum, the modified Nuss procedure appears to be a useful technique for simultaneous surgery with the TCPC Fontan procedure.
Author Contribution
Hisashi Yoshida, Tai Fuchigami and Yusuke Iwata conceived the idea of this implantation and contributed to the interpretation of data. Hisashi Yoshida drafted the original manuscript. Yusuke Iwata supervised the conduct of this case. All authors reviewed the manuscript draft and revised. All authors approved the final version of the manuscript to be published.
 ,Yusuke Iwata,Tai FuchigamiHisashi Yoshida
,Yusuke Iwata,Tai FuchigamiHisashi Yoshida